
Hindfoot Nail Fusion
TibioTalarCalcaneal (TTC) Fusion
Mr Williams is a consultant orthopaedic surgeon specialising in foot and ankle surgery in Colchester. Find out more about Mr Williams.
Print / Download this Page
A Tibiotalarcalcaneal (TTC) fusion involves fixing/fusing together the ankle joint and the subtalar joint (Underankle) at the back part of the foot such that they become solid, removing the arthritis and never move again.
Much like a fracture unites so the bone should grow across between the bones (Calcaneus to talus to tibia) becoming one solid structure.

Xrays & diagram showing metal rod and screws across ankle and subtalar joints securing a Tibiotalarcalcaneal Fusion (Images from Google - http://www.boneschool.com/lower-limb/foot-and-ankle/ankle-arthrodesis)
Tibiotalarcalcaneal (TTC) Fusion is a recognised treatment for improving the chronic pain of arthritic hindfoot and ankle joints, it can also be used for correcting deformity. It is considered in the situation where all sensible and practical non-surgical methods have failed to provide or sustain adequate quality of life with respect to pain and mobility related to the joints to be fused.
Expectations of a Tibiotalarcalcaneal (TTC) fusion
A successful TTC fusion should provide significant improvement in pain and therefore mobility.
Tibiotalarcalcaneal fusion has been shown to technically work in up to 75-85% of cases. This mirrors in a patient satisfaction rate of similar ball-park figures. It is not a perfect operation restoring normality.
Stopping these joints from moving causes stiffness in this part of the foot and ankle.
Your walking gait will be altered as you lose all ankle movement. However your overall mobility should be better as the pain is much improved. The loss of subtalar movement once fused can also mean an unsteadiness when walking on uneven surfaces long term.
Physiotherapists will help you regain a new walking pattern and an Orthotist will help with shoewear advice and modifications as necessary.
- An example of this is the rocker bottom shoe such as MBT or Skecher’s “Shape-Ups”.

A Rocker Bottom Shoe e.g. Skechers ‘Shape-ups’
The Hindfoot Nail (TTC) Operation itself
- During the operation skin cuts will be made in appropriate positions to allow access to the joints that need to be fused.
- To access the ankle the end of the fibula bone (outer ankle bone) is cut out and used for autogenous bone graft later in the procedure.
- Once the joints are accessed all the damaged cartilage is removed to expose healthy bone underneath.
- This removes the joint and stimulates the surface bone to behave as it would if broken and start to heal the joint together by making new bone.
- Metalwork is placed into the bones to secure and compress the old joints together and hold them in position while they unite / fuse together.
- This usually done with the Nail pictured above but occasionally plates and screws are used as well or instead.
- X-rays are used during the operation to determine that the position of the bones and the screws are correct.
- The metalwork usually stays in the foot for the rest of your life.
- Your leg is placed in a ½ cast ‘Backslab’ and the wounds closed.
A surgical technique video showing the principle techniques is available on the below hyperlink
What is the ‘standard’ Hindfoot Nail Fusion recovery like?
- Tibiotalarcalcaneal fusion is performed as an inpatient procedure and usually under a General anaesthetic unless there are medical reasons to avoid this.
- It takes between 2- 3 hours to do.
- You will stay in for 1-2 nights, occasionally longer.
- You will need someone to take you home.
- You will need an adult with you in the house for the initial 3 days after going home.
- You will require regular tablet painkillers for first 1-2 weeks
- You may have some thigh discomfort or bruising from the pressure of the tourniquet (300mmHg) used during the surgery. This will usually settle in few days or weeks
- We use x-rays during the operation. We know that pregnant women are at risk from the use of x-rays and therefore we ask
**If there is any chance you may be pregnant at the time your procedure is due you must inform us before your operation.**
What about walking after Tibiotalarcalcaneal Fusion?
- You will be using crutches / walking frame to mobilise during the first few weeks. Very occasionally you might require a wheelchair.
- After the operation your foot will be wrapped in a ½ plaster cast (Backslab) and should be comfortable with the use of tablet painkillers when you go home.
- Weight bearing after Hindfoot Nail Fusion:
- Your instructions regarding will be discussed with your surgeon.
- Usual regime:-
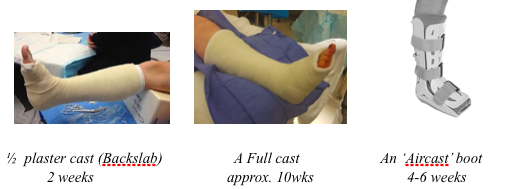
- 4 weeks Non-weightbearing in cast
- 4 weeks Partial weightbearing in full cast
- 4 weeks Full weightbearing in full cast
- 4-6 weeks Full wightbearing in ‘aircast’ Boot
- Usual regime:-
- Your instructions regarding will be discussed with your surgeon.
- Usual Follow up Appointments
- 1st appointment at 1 week = Wound check appointment
- Checking for signs of infection.
- 2nd appointment at 2 weeks = Wound check appointment
- Change to full cast
- 3rd appointment at 8-10 weeks = Fusion progression appointment
- You will likely have an x-ray at this stage
- 4th appointment at 12 weeks = Progress to removable ‘aircast’ boot
- You will likely have a second x-ray at this stage
- You may begin to move the foot at this stage
- 1st appointment at 1 week = Wound check appointment
- Physiotherapy = The timing of this varies but is usually reserved for when you get out of the cast and begin weaning from the boot.
- Driving –
- Right foot surgery = No driving until out of Boot / Cast
- Left foot Surgery = No driving for 3 weeks. Subsequently OK if comfortable and in Automatic car
- IF IN ANY DOUBT ABOUT YOUR ABLILTY TO SAFELY CONTROL THE VEHICLE DO NOT DRIVE
- Returning to work is a minimum of 3 weeks to allow wound healing & swelling to settle but can be longer depending. Afterwards should be discussed with the team.
For various reasons, during Hindfoot Nail fusion, its recovery or even recognised before we start , it may be necessary to stay in a full cast for over 12 weeks or more after the surgery. This will always be discussed and explanation provided.
What are the downsides to tbiotalarcalcaneal fusion surgery?
With the ankle and subtalar joints fused together the other joints in your foot and knee have to adapt and perform movements or functions they were not expecting or designed to do. Therefore:-
- If you have any pains from joint arthritis in other parts of your foot or knee they may worsened by a hindfoot fusion.
- In the long term the excessive stress on normal surrounding joints can cause them to develop arthritis. This can take years but on occasions can occur more quickly.
- Your leg may be slightly shorter than the otherside but noticeable and require a small build-up of the sole of a shoe to accommodate this.
What are the Alternatives to Tibiotalarcalcaneal Fusion?
These should be discussed with your surgeon but they include:-
- Footwear modification – usually provided in conjunction with the Orthotic department modification to footwear and the way the foot moves can sometimes help to improve pain or function to the point where the symptoms are acceptable and surgery is not needed.
- Injections – Many people will have a Cortisone injection before they go on to be recommended a fusion. These are done with x-ray in the operating theatre for accuracy and can help with diagnosis and have a variable effect on pain. Some people get long term relief for months and some only a very short period of improvement.
- Bracing – Any brace that restricts the stabilising motion of the hindfoot (wigwag/side to side) and ankle will help calm the pain experienced.
- On-going conservative Treatment - Fusion is a quality of life improving procedure and you can of course decide to avoid the surgery at any point. This may be in conjunction with the General practitioner (GP) or a specialist pain team.
- Subtalar Fusion and Ankle Replacement - Usually performed as staged procedures some patients are suitable for this more drawn out ambitious plan of care. In certain instances it can be appropriate to consider having a subtalar joint fusion followed 3-6months later by an ankle replacement. This will be discussed.
What are the Risks of Hindfoot nail ? Tibiotalarcalcaneal fusion Surgery?
This surgery carries risks as we have to cut through your skin work on the bones inside your foot & ankle. Metalwork implants are also put in to secure the bones together. The incisions are kept as small as possible to minimise these risks while being large enough to safely perform the operation.
Never the less there remains the risks of:-
Bleeding / vascular injury– This is usually minimal and settles with rest and elevation. If it continues leaking out of the dressing you should seek medical help
Infection –
Superficial skin infection around the stitches can be managed with some antibiotics and rarely affects the overall outcome.
Deep infection in the bone is more serious, can have a sustained effect on the outcome and occasionally require more dramatic surgery such as redoing the operation or in extreme and very rare circumstances amputation.
Nerve damage/ Neuritis - The surgical wounds pass near nerves that supply sensation to your foot. Immediately after the surgery the scars and even foot can be a little numb and tingly. This usually resolves by about 6 weeks. Very occasionally it can be permanent with either loss of feeling, ‘pins and needles’ or a chronic ‘nerve’ pain occurring.
Tendon Damage –The wounds pass very near the tendons that traverse the foot. Whilst naturally being careful there remains the inherent risk of slight damage to these tendons which can result in pain or rarely rupture. Any pain or new onset foot/ toe weakness – seek medical attention
Delayed Union - – Despite a surgeons best efforts, this operation relies on your body growing new bone across the hindfoot joints. Occasionally this takes longer than usual requiring a cast or boot for further weeks to months. Smoking severely impair this process and it is therefore vital that you do not smoke or use nicotine replacement during your recovery.
Non-union – Despite a surgeons best efforts, this operation relies on your body growing new bone across the hindfoot joints. This occasionally does not happen and a scar tissue (fibrous joint) forms instead. It presents as ongoing pain after the operation and can be seen on an Xray or Scan. If symptomatic the operation can occasionally have to be re-done. Again smoking and Nicotine have a large impact here.
Metalwork Problems – Internal screws, clips and plates can be used to hold the bones compressed together at the end of the operation.
They are designed to stay in forever.
They are made of Titanium or Stainless steel
If you are allergic / sensitive to any metals– PLEASE LET THE TEAM KNOW BEFORE THE SURGERY.
Occasionally the metal can be prominent under the skin and you may request for them to be removed later in the year once fusion is complete.
Despite a surgeons best techniques occasionally the tips of the screws can puncture into a neighbouring joint and cause damage or pain such that they require removal.
Metalwork can break during or after an operation and a surgeon will use their judgement to decide whether it is better removed or left if causing no harm.
Joint Malposition - The aim of the surgery is to set the joints with your foot ‘square’ to the floor using both xray and experience to achieve this. Malposition can result in walking problems that require revision treatment to rectify it.
Foot Joint pains – As mentioned previously the extra requirements placed on the foot joints can exacerbate or even cause arthritis in the foot in the medium or long term. Occasionally it can be sooner.
Complex Regional Pain – Any operation on the foot or ankle seems to carry a small chance of this difficult and frustrating pain condition. It is usually not clear why it happens and there is little to predict it. Though rare this chronically painful problem can be life affecting.
Asymmetric Gait effects - Following surgery you may well use crutches or a stick and latterly walk differently. This can in turn affect you as a whole, aggravating your back or other leg. Usually short lasting and settling early, occasionally it can last. If you experience this please inform your physiotherapist who can assist in rehabilitation.
Leg length discrepancy – Because cartilage and bone are necessaryily removed from the joints to get fusion some height is lost. Usually the difference is negligible but on occasions the difference needs to be made up in footwear modification with a thickened sole for example.
Thrombosis – (Deep Vein Thrombosis / Blood Clot / Pulmonary Embolism). Any operation on the leg places you at slight risk of this. A thrombosis can occur in the leg muscle veins causing pain and swelling. Pulmonary Embolism (PE) is where the leg thrombosis moves and traps in the lung which can be fatal.
- If you develop calf pain and / or swelling that doesn’t go away with rest and elevation – seek medical attention
- If you develop sudden shortness of breath or chest pain – Seek Medical attention
- To mitigate against it you should:
- drink plenty of water
- Keep all joints moving, especially knee and ankle (within confines of bandages)
- Wear a thrombosis prevention stocking (TED) which will be provided by the hospital.
- Take a small injection of Enoxaparin every evening that you self administer for the entire duration you are in cast.
-
- If you or a family member have ever had a thrombosis please let the medical or nursing staff know before the surgery
GENERAL RISKS OF ANY SURGICAL PROCEDURE
- Small areas of the lung may collapse, which increases the risk of a chest infection.
- If you develop shortness of breath or start coughing up blood or yellow sputum – Seek medical attention
- Stress of surgery can cause a heart attack or stroke.
- If you develop chest pain / sudden weakness or collapse - Seek medical attention
- Immediate life-threatening events may occur during any surgical procedure, which may require life saving interventions.
- Increased risk of wound infection, heart and lung complications, and thrombosis are associated with OBESITY and/or SMOKING.
What should I do if I have a problem after the operation?
If you experience any of the following you should contact the hospital team and seek advice.
- Increasing pain despite your painkillers
- Increasing leg or foot swelling despite rest and elevation,
- Sudden chest pain or shortness of breath
- Redness or oozing of blood or pus
- High temperature or Fever
Please write questions you may have down and the whole team will always be happy to answer them prior to proceeding with any surgery.
I hope this guide has given you some insight into the procedure and I’m sure you understand that nothing n this style of work is exact or absolute and just is the basis of my practice. I will of course adapt the above your to you individual case and requirements and work with you for the best outcome.
All example Images taken from www.google.com.
Print / Download this Page
Next Steps...
If you would like to arrange a consultation to discuss your foot or ankle problems with Mr Williams, then please contact us.